Önder Ergönül on Ebola Outbreak
 Since late spring of this year, we have been hearing two words in almost every news program; “Ebola" and "outbreak." Because of the importance of the subject, the editorial team of The Bridge, seeks to inform our membership body about Ebola virus outbreak. We reached Dr. Önder Ergönül, a professor of infectious diseases and clinical microbiology at Koc University and asked him some of the frequently asked questions. Below is our conversation with Dr. Ergönül.
Since late spring of this year, we have been hearing two words in almost every news program; “Ebola" and "outbreak." Because of the importance of the subject, the editorial team of The Bridge, seeks to inform our membership body about Ebola virus outbreak. We reached Dr. Önder Ergönül, a professor of infectious diseases and clinical microbiology at Koc University and asked him some of the frequently asked questions. Below is our conversation with Dr. Ergönül.
In addition to his faculty position at Koc University, Dr. Ergönül is also the chair of Infectious Diseases Department of American Hospital in Istanbul, and Turkish Society of Infectious Diseases and Clinical Microbiology. He is a full member of the Turkish Academy of Sciences.
The Bridge: Dr. Ergönül, thank you very much for taking the time to answer our questions about ebola epidemic that started in West Africa, and now seems to be spreading to other countries including the United States and Spain. Would you please give us a brief history of the Ebola virus epidemic, and talk about the current status of the epidemic?
Önder Ergönül: Ebola virus first discovered in 1976 in Africa, and since then every year hundreds of people were infected and almost 90% died. This is a disease that is known for its very high fatality. Ebola first appeared in 1976 in two simultaneous outbreaks, in Nzara, Sudan, and in Yambuku, Democratic Republic of Congo (DRC). From 1976 to December 2012 a total of 23 outbreaks or isolated cases of Ebola have been reported; during these events a total of 2388 Ebola cases including 1590 deaths were reported (WHO fact sheet, no 103, 2012). By the year 2014, we are in the middle of the largest outbreak of Ebola. By October 25, number of the cases was reported to be more than 10,000 (laboratory confirmed 5,700) and nearly 5,000 deaths.
Since its discovery in 1976, Ebola virus disease (EVD) has mostly occurred in sub-Saharan Africa. Sudan, Democratic Republic of Congo, Gabon, Uganda, and Republic of the Congo have reported EVD epidemics. Some countries report serologic evidence of Ebola infection among animals and humans, Guinea, Sierra Leone, Liberia, Nigeria, Cameroon, Chad, Central African Republic, Ethiopia, and Madagascar. By the year 2014, now the most of the cases were reported from Guinea, Sierra Leone, Liberia, Nigeria, and Senegal.
T. B. : I would like to give our readers some information about the Ebola Virus. Could you tell us about the virus; where it was originated, how it is evolved and how it is transmitted among people?
O. E. : Ebola is first introduced into the human population through close contact with the blood, secretions, organs, or other bodily fluids of infected animals such as chimpanzees, gorillas, monkeys, forest antelopes, fruit bats, and porcupines found dead or ill in the rain forest. It is not always possible to identify the source of primary human infection. In Africa, fruit bats, particularly species of the genera Hypsignathus monstrosus, Epomops franqueti, and Myonycteris torquata, are considered possible natural hosts for Ebola virus. Secondary human-to-human transmission spreads in the community resulting from close contact with the blood, secretions, organs, or other bodily fluids of infected people. Burial ceremonies where mourners have direct contact with the body of the deceased person can also play a role in the transmission of Ebola. Transmission via infected semen can occur up to 7 weeks after clinical recovery.
Healthcare workers have frequently been infected while treating Ebola patients. This has occurred through close contact without appropriate infection control precautions and adequate barrier nursing procedures. For example, healthcare workers not wearing gloves and/or masks and/or goggles appropriately and who are exposed to direct contact with infected patients’ blood are at risk. Using barrier precautions appropriately is important. These are simple precautions, but we cannot say that always adequate and easy to adhere.
Handling and preparation of food may also be another unapparent route of transmission.
T. B. : Those of us who read the novel "Hot Zone" by Richard Preston may recall the gruesomeness of the Ebola infection. But would you tell us about the progression of the disease as an expert on viral diseases and a medical professional?
O.E. : Such books are good and definitely beneficial, at least to tell about what scientific discoveries are. They also carry the risk of unrealism. First, virus enters to the body, and then flu like illness starts, including high fever, headache, muscle aches, nausea, vomiting and diarrhea. After these symptoms (prodromal period), bleedings from various sites start. Bleeding could be from anywhere. Mainly from mouth and nose, but also could be from gastrointestinal tract, or into the internal organs. We still do not know, who are more prone to bleeding. Some people have more severe disease than the others. Interestingly, people perceive that all the infected individuals with Ebola will eventually die. No, fatality rate is between 50-70%.
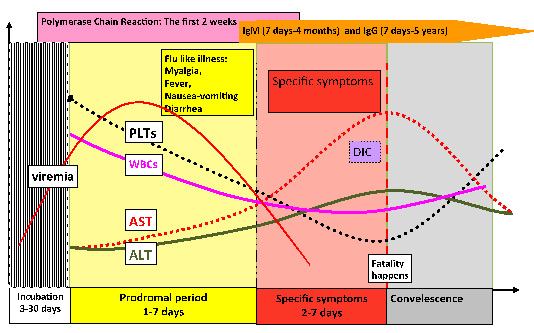
Ergonul, 2006 and 2012
T. B. : I want to focus on the transmission of the virus a little more. Because recently we have been witnessing a hype in the regular and social media on the epidemic, consequently some myth is mixed with the facts. For example if we are in a plane with a patient who is infectious, can we catch the virus? Is there a danger of Ebola spreading in the US or Turkey?
O. E. : The basic reproduction number of infection was calculated around 2 (N Engl J Med, September 23). Basic reproduction number gives the average number of people, who could be infected from an infected individual. We should accept that this number is a very rough approximation, however in Ebola example tells us that the dissemination will not be so much. The main risk for the people, who lives outside of epidemic zone, is contact with blood and body fluids of the infected people. If everyone can protect himself or herself appropriately, the risk is very low. In airplanes or similar such places that we could be present together with infected people, the most important measure is the hand hygiene and self hygiene. Virus can stay alive for 7-8 hours on dry surfaces. Carrying disinfectants could be a good idea.
T. B. : How is the infected individuals treated? What is the rate of recovery or death?
O.E. : There are 4 candidate drug trials against the virus, but they are not ready yet. With the best scenario, they will be ready for the next outbreaks. Supportive treatment is important. This means replacing the blood and blood products, fluid and electrolytes. Support in a well equipped intensive care unit could be live saving.
T. B. : What can we do to protect ourselves against Ebola infection.
O. E. : First of all, the people who live out of the epidemic zone, should not exaggerate the risk of transmission. Transmission can only be possible after contact with infected animals or humans. This can occur in epidemic zone. Again, the most important measure is the hand hygiene and self hygiene. Carrying disinfectants in our bags or purses would certainly help.
T. B. : Thank you very much for this valuable information.
(Not: Dr. Ergönül also provided the following information for those of our readers who are interested in learning more about the virus itself: Ebola virus is a single stranded RNA virus. As a disease entity it is classified among viral hemorrhagic fevers. Genus Ebolavirus is one of the three members of the Filoviridae family (filovirus) together with genus Marburgvirus and genus Cuevavirus. All are enveloped, single-strand, negative-sense RNA viruses. Genus Ebolavirus is comprised of five distinct species: species Bundibugyo ebolavirus, virus: Bundibugyo virus (BDBV); species Zaire ebolavirus, virus: Ebola virus (EBOV); species Reston ebolavirus, virus: Reston virus (RESTV); species Sudan ebolavirus, virus: Sudan virus (SUDV); and species Taı¨ Forest ebolavirus, virus: Taı¨ Forest virus (TAFV). BDBV, EBOV, and SUDV have been associated with large Ebola virus disease (EVD) outbreaks in Africa, whereas RESTV and TAFV have not).
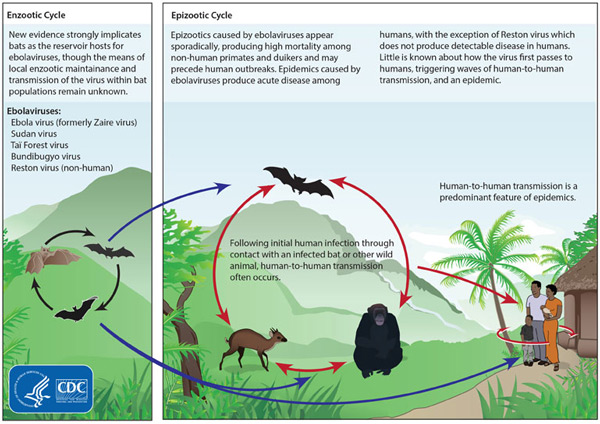
Life Cycle of Ebola Virus (Source: Center for Disease Control)